Medicines, here are the government's objectives with the Grillo plan. Speak the prof. Garattini
di Chiara Daina – Start Mag – 27 dicembre 2018
All the guidelines of the Ministry of Health directed by Giulia Grillo with a new pharmaceutical governance according to Professor Silvio Garattini, illustrious pharmacologist and founder of the Mario Negri Institute
The National Health Service is not obliged to include in the list of medicines which reimburses all those used to treat the same disease, even if they have different active ingredients. But only the molecules that prove to have a more advantageous risk-benefit and cost-benefit ratio. This is the assumption underlying the planning document of the new pharmaceutical governance presented on 10 December by the Ministry of Health.
HERE ARE THE GOALS OF THE GOVERNMENT ON DRUGS
“The goal is first of all to rationalize the use of drugs, which will necessarily lead to a reduction in spending - highlights Silvio Garattini, the illustrious pharmacologist and founder of the Mario Negri Institute, who participated in the technical table on drugs - If the While offering the same drugs, albeit under different names, prescriptions are also increasing as each company tries to push its own product to market. The European Medicines Agency – explains Garattini – evaluates the molecule according to three criteria: quality, efficacy and safety; instead we must also consider the added therapeutic value. Medicines are not consumer goods, but health tools”.
THE ANALYSIS OF THE GARATTINI PHARMACOLOGIST
In fact, the market is saturated with duplication. “We cannot have 21 antidepressant drugs in Italy and not know if there is one that works better than the others – continues the pharmacologist – The same goes for painkillers or gastroprotectors. And it is not acceptable that the NHS spends 280 million a year on vitamin D which does not change the number of falls or fractures in the elderly".
THE STRATEGY IN ACTION

THE ROLE OF THE REGIONS
To move from theory to practice, the Regions must also do their part by encouraging competition in tenders for the purchase of hospital medicines. “The national handbook represents an aid and a guide for all regions, the problem is to govern it at the local level. As if to say, it is not the list of things to do that is missing, but the control room to apply them". The virtuous mechanism of purchases by therapeutic equivalence must therefore be triggered, as suggested in the document on the new pharmaceutical governance. "The region - explains Marata - should first make a list of drugs with the same therapeutic indication, submit it to the evaluation of the Aifa technical-scientific commission, and then ban the tender to obtain greater savings". A method introduced in 2012 with the Balduzzi law but still little used.
THE GUIDELINES FOR A NEW PHARMACEUTICAL GOVERNANCE
In the guidelines for reforming pharmaceutical governance, with a view to economic sustainability, AIFA is also asked to promote information campaigns to raise awareness for doctors and patients, on the use of generic and biosimilar drugs, comparable in terms of efficacy and safety to the original ones. “It is not clear why in the southern regions, where there is sun and sea, more drugs are prescribed and the percentage of expenditure for those covered by a patent is higher than in those in the North – comments Garattini -. In Lombardy, for example, the use of generic drugs stands at 37.2 per cent, while in Calabria at 15.8”.
THE PLAN ON DRUGS
Another point on which the sector reorganization plan insists is the dispensing of drugs with a number of personalized doses, "as is already the case in England and the United States" recalls the pharmacologist. "Let's think of antibiotic packs - he gives an example - they almost always remain after the therapy and the risk is that, by remaining around the house, they are taken inappropriately, or expire". Another request is to promote research independent of Big Pharma funding and equally interest-free scientific information. “Today information is asymmetrical – concludes Garattini – because it is the industries that make it; instead Aifa must take care of it, as it once did, with the distribution to doctors of a pharmacological manual and a periodical with all the indications ".
Extract from an article published on Ilfattoquotidiano.it
Editor's note:
We read in the Fatto Quotidiano: “It is not clear why in the regions of the South, where there is sun and the sea, more drugs are prescribed and the percentage of expenditure for those covered by patents is higher than in those of the North - comments Garattini -. In Lombardy, for example, the use of generic drugs stands at 37.2 per cent, while in Calabria to 15.8” (Daily fact)
A statement that the great drug scientist should verify and a scientist then should not be prejudiced.

More people die in the southern regions. So much so that being born in Southern Italy, for example in Campania, means living on average 3-4 years less than those born in Trento. Ricciardi (ISS) identifies various factors on the lower life expectancy in the south: "Poor prevention, starting from the lower response to cancer screening, later diagnoses, lower availability of innovative drugs and lower efficacy and efficiency of health facilities". But it is also the styles and quality of life that weigh, such as the presence of factories of death. see ILVA, CERANO, Petrochemical of Gela and we could continue with the waste from the north buried between Campania and Southern Italy. To this we add that many citizens are poor or unemployed and go to the doctor to get a prescription even for drugs for a few euros, something that doesn't happen in the north.
Se poi il sole e il mare evitano la prescrizione di farmaci perché sono tutti più sani, non si capisce come mai nel Mozambico, dove c’è sia il sole che il mare, la speranza di vita media è di 41 anni tra la popolazione maschile e di 40 anni tra quella femminile.
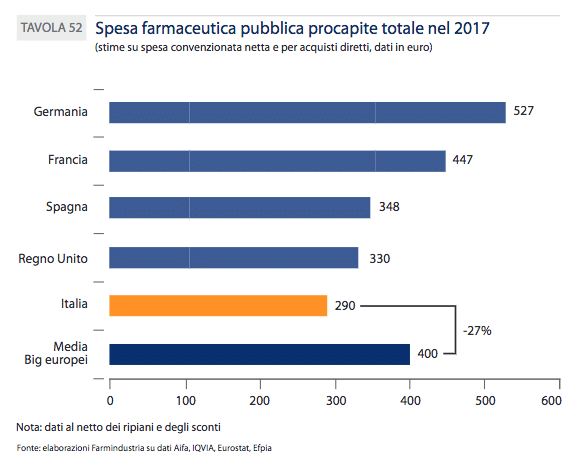
Non va inoltre nemmeno dimenticato che in Italia l’uso dei farmaci pro capite è il più basso rispetto ai 5 maggiori Paesi dell’UE.
Related news: ISTAT confirms: in 2015 never so many deaths since the war. Health care cuts?
Life expectancy decreases, people die more in the South
FNOMCeO. Doctor, is it true that… Does poverty make you sick?