
9,5% of Italians give up treatment for economic reasons or too long waiting lists. But the 71,5% judges the performances received as excellent. Compare expenditure, response to needs, staffing and patient satisfaction. What emerges is a country substantially divided between a health system in the North that works and one in the South (including Lazio) in difficulty. More serious situation in the regions in the repayment plan. The southern regions are the most "underfinanced". THE 2015 ANNUAL REPORT.
May 20, 2015 – the online pharmacist
20 MAY - Below is the complete chapter of the 2015 Istat Annual Report dedicated to the "Territorial heterogeneity of the National Health System: allocative equity and levels of satisfaction”.
 The reforms that have affected the National Health System (NHS) since the 1990s - up to the latest provisions on expenditure containment and the Health Pact - have had a threefold objective: that of implementing the principle of subsidiarity in the health sector, through the devolution to the Regions of the management and organization of assistance services and the introduction of fiscal federalism; start the process of corporatization of healthcare facilities; improve the efficiency of the sector, through expenditure control and the obligation of the Regions to balance the budget.
The reforms that have affected the National Health System (NHS) since the 1990s - up to the latest provisions on expenditure containment and the Health Pact - have had a threefold objective: that of implementing the principle of subsidiarity in the health sector, through the devolution to the Regions of the management and organization of assistance services and the introduction of fiscal federalism; start the process of corporatization of healthcare facilities; improve the efficiency of the sector, through expenditure control and the obligation of the Regions to balance the budget.
The debt repayment process, which many Regions have had to face, associated with the difficult economic situation, has resulted in a reduction in equity in access to the treatments which inspire our NHS. The fact that some of the Regions under the debt repayment plan are unable to ensure the essential levels of assistance, providing volumes of services below the standards deemed adequate, testifies to the difficulties of the sector.
The analysis that follows focuses on the allocative aspects of the System and on the congruence with the potential needs of health care. To this end, a comparison was made between the "geography of health", the map of the health personnel endowment (proxy of the presence of structures in the area) and the map of NHS funding. The comparison between the clear north-south territorial gradient in the distribution of funding between the Regions and the much more varied geography of health highlights the imbalance between the potential needs for health care and the criteria for allocating the resources adopted.
In the southern regions the per capita share of financing does not reach 1,900 euros, with the minimum of 1,755 in Campania, while in other areas of the country it exceeds two thousand euros. The maximum values, exceeding 2,300 euros, are found in Valle d'Aosta, Bolzano and Trento, where the average endowments of healthcare personnel are also higher against a clearly lower prevalence of population in poor health conditions.
High shares of people with health problems (more than a fifth of the total population) are found in Umbria, Sardinia, Emilia-Romagna, Marche, Friuli-Venezia Giulia, Puglia and Abruzzo.
T among these, a critical situation is observed for the Regions in the recovery plan who have low levels of health personnel and receive funding lower than that correlated to need (1,810 euros per inhabitant in Puglia, 1,890 in the Marches and 1,915 in Sardinia); this long-standing imbalance could be a cause as well as an effect of budget deficits. The number of health personnel and the amount of public funding are important elements of evaluation but, in such a complex and articulated framework, it is essential to measure the offer of health services also in terms of quality perceived by citizens and accessibility of assistance .
among these, a critical situation is observed for the Regions in the recovery plan who have low levels of health personnel and receive funding lower than that correlated to need (1,810 euros per inhabitant in Puglia, 1,890 in the Marches and 1,915 in Sardinia); this long-standing imbalance could be a cause as well as an effect of budget deficits. The number of health personnel and the amount of public funding are important elements of evaluation but, in such a complex and articulated framework, it is essential to measure the offer of health services also in terms of quality perceived by citizens and accessibility of assistance .
The patient's perspective is in fact recognized as an important element for assessing the quality of care, because it allows consideration of aspects of the care activity that would otherwise not be evaluated, such as communication, transparency, sharing of therapeutic decisions and respect for the dignity of the person.
To respond to this objective, the overall level of satisfaction of citizens with the public health service and the specific level of the services provided in both public and accredited structures was considered, as well as the possible waiver of health services provided by the NHS for economic reasons or reasons related to the offer (waiting lists too long, inconvenience to reach the facility or inconvenient times for using the service).
 The majority of the adult population (60.8 percent) positively evaluated the public health service, with the attribution of scores ranging between 6 and 10.23 stable evaluation compared to 2005. However, the overall judgment hides territorial inequalities, which have increased compared to 2005.
The majority of the adult population (60.8 percent) positively evaluated the public health service, with the attribution of scores ranging between 6 and 10.23 stable evaluation compared to 2005. However, the overall judgment hides territorial inequalities, which have increased compared to 2005.
In the North, the share of citizens who consider the activity of the public health service very satisfactory is increasing: almost 30 per cent declare themselves very satisfied (with scores from 8 to 10). In the South the share does not reach ten per cent. Judgments have polarized over time, with the overall increase of very satisfied people in the North and very dissatisfied people, especially in the South, where almost one person out of three expresses a negative opinion (with scores from 1 to 4).
In Lazio – one of the regions with a particularly onerous repayment plan – there is a clear increase in the share of dissatisfied people, equal to 8 percentage points. With the same social and demographic characteristics and the main socio-economic determinants, the strong imbalances in the geography of satisfaction are confirmed.
The opportunity to have a high level of satisfaction with respect to Tuscany (taken as a reference because it is similar to the national average) is over four times higher than in Bolzano and Trento and three times higher in Valle d'Aosta; it halves in almost all the regions of the South and in Lazio. The analysis by Local Health Authority (Asl) makes it possible to evaluate the high territorial heterogeneity in detail. In some Local Health Authorities, for example those of Bolzano and Trento, the share of very satisfied represents the majority of the adult population (54.2 and 51.6 percent respectively), while the lowest percentages are found in some Local Health Authorities in Campania (2 .3 per cent) or Calabria (about three per cent).
The regions with the greatest internal heterogeneity are Piedmont, where the share of very satisfied varies in the 13 Local Health Authorities from 14.7 to 43.6 per cent, and Tuscany, where it varies from 8.7 to 32.3 per cent.
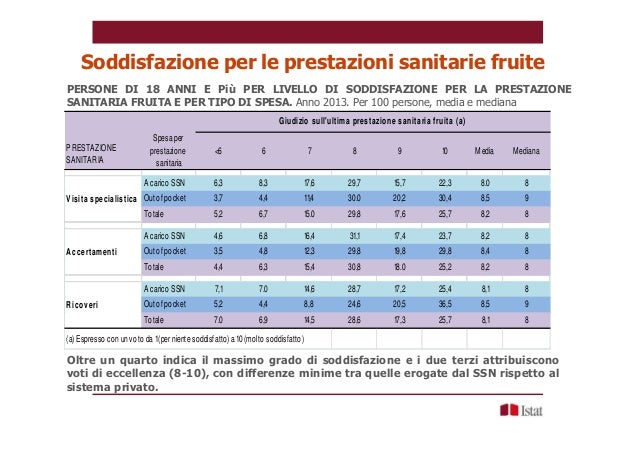
The level of satisfaction significantly improves when the assessment concerns health services used within the framework of the NHS.
71.5 per cent of those who attended a specialist visit or assessment expressed an opinion of excellence on the overall quality of the last service, with scores between 8 and 10.26 The estimate refers to a large group of the population: around 25 million people, 41.2 per cent of the population, had recourse to specialist medical examinations (excluding dental ones) or specialist diagnostic checks paid for by the NHS.
 The territorial differences in the level of satisfaction are less pronounced than those for the overall opinion on the NHS, above all as a result of higher values in the South. In fact, even in the regions that are in the lowest part of the ranking (Molise, Campania, Calabria), the majority of those who have undergone a visit or a specialist assessment by the public health service assign a score ranging from 8 at 10.
The territorial differences in the level of satisfaction are less pronounced than those for the overall opinion on the NHS, above all as a result of higher values in the South. In fact, even in the regions that are in the lowest part of the ranking (Molise, Campania, Calabria), the majority of those who have undergone a visit or a specialist assessment by the public health service assign a score ranging from 8 at 10.
Despite this, the distance of the North from the regions of the South and from some of the Center remains evident. We are more often very satisfied with visits or specialist checks in Trento (with a relative risk almost double compared to Sardinia taken as a reference), in Bolzano, in Emilia-Romagna and Lombardy, while lower levels are observed in the southern regions but even in much of the Center.
In all local health authorities, with the exception of five cases, the majority of those who have undergone specialist visits or checks assign excellent scores.
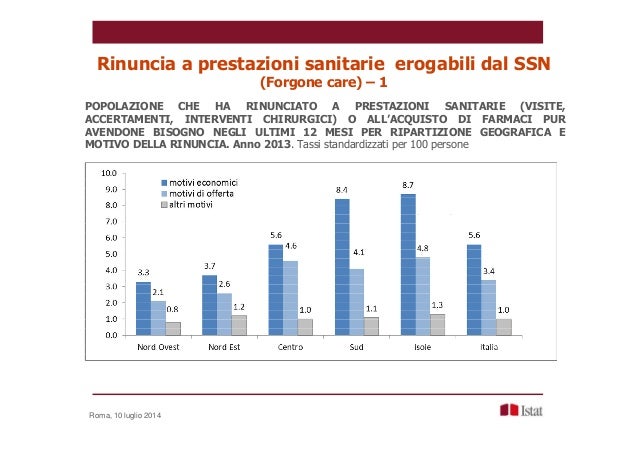
The phenomenon of renunciation of health services (foregone care) is an important indicator of the quality of the supply, because it reveals a demand for assistance to which the system is unable to give an adequate response.
9.5 per cent of the population was unable to benefit from services that should be guaranteed by the public health service for economic reasons or for lack of supply structures (waiting times too long, difficulty in reaching the structure or inconvenient hours).
The weaknesses are concentrated, once again, on some subjects and on specific areas. The lowest share (6.2 per cent) of renunciations for economic reasons or lack of supply is recorded in the North-West, while in the South and Islands the share is more than double (13.2 per cent). However, the disadvantage for those with a less favorable economic condition is greater in the North.
Observing the regional differences, keeping under control the socio-demographic characteristics and the other factors that have an impact on the phenomenon, a clear separation emerges between the Centre-North and the South to the detriment of the latter. The exception is Lazio, which presents a risk 60 percent higher than the reference region, confirming a decidedly worse situation than the other central regions. The lowest risk of renunciation is found in the autonomous provinces of Trento and Bolzano, in Valle d'Aosta and in Lombardy.
T There are considerable distances between the Local Health Authorities: we go from 21.7 per cent of waivers in one Local Health Authority of Sardinia to 2.6 per cent in the Local Health Authority of Trento and in one of Lombardy. In the North there is the greatest concentration of Local Health Authorities which have shares of no more than 5.5 per cent of people who renounce services payable by the NHS for reasons linked to the offer. In any case, the intra-regional heterogeneity deserves particular attention, which presents a maximum value in Emilia-Romagna (from 2.9 to 13.7 per cent, among the 11 Local Health Authorities), high in Piedmont, Tuscany, Lazio, Sicily, Puglia and Sardinia, while in Veneto, the region with the highest number of Local Health Authorities, the renunciation of essential services fluctuates between 4.0 and 11.5 percent.
There are considerable distances between the Local Health Authorities: we go from 21.7 per cent of waivers in one Local Health Authority of Sardinia to 2.6 per cent in the Local Health Authority of Trento and in one of Lombardy. In the North there is the greatest concentration of Local Health Authorities which have shares of no more than 5.5 per cent of people who renounce services payable by the NHS for reasons linked to the offer. In any case, the intra-regional heterogeneity deserves particular attention, which presents a maximum value in Emilia-Romagna (from 2.9 to 13.7 per cent, among the 11 Local Health Authorities), high in Piedmont, Tuscany, Lazio, Sicily, Puglia and Sardinia, while in Veneto, the region with the highest number of Local Health Authorities, the renunciation of essential services fluctuates between 4.0 and 11.5 percent.
Allocative imbalances, the contraction in spending and the consequent difficulties in guaranteeing the essential levels of assistance referred to can translate into an increase in household spending (out of pocket). In fact, the main tools that the Regions implement to contain spending and reduce debt are the introduction of co-payments and share-sharing of expenditure by citizens. These are interventions that have the objective of reducing public expenditure, also through a containment of demand obtained with the introduction of a cost for health services.
However, further expenditure increases for families could increase the renunciation of health services, often due to economic reasons. This entails a risk of sanitary under-consumption, dangerous for the health conditions of the population
Related news: OECD. Italy in 17th place out of 36 countries for perceived state of health. Life expectancy at 82 years, the 66% declares itself to be in good condition – (OECD Economics Surveys ITALY)
Related news: The Ssn towards 'The perfect storm'. Here's why we're close to 'shipwreck' and how to get out of it 'alive' .
Our National Health Service is one of the best in the world: it has in fact ensured Italians a good overall level of health, responding, over time, to the health care expectations of all citizens. And yet, also thanks to the recent international economic and financial crisis, a possible 'perfect storm' is looming on the horizon which risks, in the absence of a significant change of course, to make it 'shipwreck'. The authors, through an objective and systematic analysis, present an articulated photograph of the history and perspectives of our 'health system': demographic and health trends, the faults of those who are 'guides' or 'on board' the ship, the alarms raised and remained unheard for years, the main structural and qualitative deficiencies. By following the logical path drawn, we can thus already see the first signs that clearly tell us that there is no time to waste. The book represents a valuable tool, not only for insiders, but also for all citizens who want to better understand what our National Health Service was, what it is and what it could be. Foreword by Beatrice Lorenzin.




